The child was apparently asymptomatic 1 year back. Then his guardians noticed that he was gaining weight. The child mentioned that he gained around 15 kgs in that one year. (from 35 kgs to 50 kgs). Along with that, he developed shortness of breath. It was grade 1 breathlessness (mMRC classification) which did not progress.
6 days back, the child developed moderate, continuous and dragging type of pain in the legs extending down from the knees bilaterally. The child's sleep was disturbed due to pain. It relieved only on medications.
There is H/o fever 2 days back which was low grade intermittent fever that subsided on medication.
There is no H/o cough, wheeze, chest pain, palpitations, syncopal attacks, dizziness
There is no H/o vomiting, headache, anorexia, burning micturition, abdominal pain or decreased urine output.
The child was admitted for evaluation.
On enquiring the background of the child, following was found out
the child's father died in an accident 5 years back and he is the only child. Since then, his grandfather has taken the guardianship. 3 years back, the child was put in a hostel since he was not doing well in studies.The child said that he adjusted well with the hostel and he has no issues.
The child mentioned that he was given some unknown tablets by his warden at his hostel whenever he injured himself during play or whenever he had fever.
Now, the patient complained that he had to skip his exams due this hospitalization.
This was the first time he was hospitalized.
The patient is not a k/c/o diabetes
There is no H/o any heart disorders, thyroid disorders, epilepsy, asthma, tuberculosis.
General Examination:
The child is conscious and cooperative and is sitting comfortably on his bed.
Child seems moderately nourished and is obese.

Clinically, there no signs of pallor, icterus clubbing or cyanosis
There is no lymphadenopathy or edema.
His Vitals were:
- BP- 100/70 mmHg in the right arm in sitting position.
- Pulse- 90 beats/min measured in the right hand. The rhythm, volume and condition of the vessel wall were normal. There are no delays.
- Temp- 98.4ºF
Mild hyperpigmentation over the nape of neck

tonsillar hypertrophy [grade 3+] (tonsillar hypertrophy)

Child has polydactyly in the left hand

Systemic examination:
Cardiovascular examination-
Precordium appears to be normal. Apical impulse is not visible.
Apex beat is palpable in the left 5th intercostal space in the mid-clavicular line, there's no tenderness, no thrills and heaves.
Jugular venous pressure is measured to be 8cm of H20.
Heart borders are normal on percussion
On auscultation, normal heart sounds are heard in Mitral, Tricuspid, Aortic and Pulmonary areas. Soft systolic murmurs [grade 2 according to Levine scale] are heard in Mitral and Pulmonary areas (Levine scale)
Respiratory examination-
Respiratory rate is measured to be 24 cycles/min.
Chest wall is normal and bilateral symmetry is maintained with breathing.
Resonant note is heard in all the lung fields on percussion
On auscultation, Vesicular breath sounds are heard in all the lung fields. there are no added sounds.
Abdominal examination-
Abdominal obesity can be appreciated. there is a rectangular scar around the umbilicus which was deliberately done as an indigenous ritual when the child was young. (Can be seen in the above picture)
No organomegaly was clinically appreciated. There's no tenderness.
Tympanic note heard in all quadrants of the abdomen on percussion.
On auscultation, Bowel sounds were heard normally.
Nervous system examination-
Higher mental functions are normal
Cranial nerves are functionally intact
Reflexes are present in all four limbs.
Motor and Sensory systems are normal
Cerebellar functions are normal.
After thorough clinical evaluation, the following investigations were ordered.

 |
| CBP |
 |
| CUE |
 |
| RFT |
 |
| LFT |
 |
| ECG |
 |
| 2D Echo |
 |
| Widal |
 |
| Routine Serology |
 |
| Thyroid profile |
 |
| Chest x-ray PA view |
After 1 day, his hemogram showed that the leukocyte counts dropped to 14,000

Plan of action:
- Tab. PARACETAMOL 500mg / QiD
- Fever charting
- Tab. Multivitamin/ OD
After two more days, the patient developed a sudden spike of fever.
the following investigations were sent after this episode
 |
| CBP |
 |
| Urine for C/S |
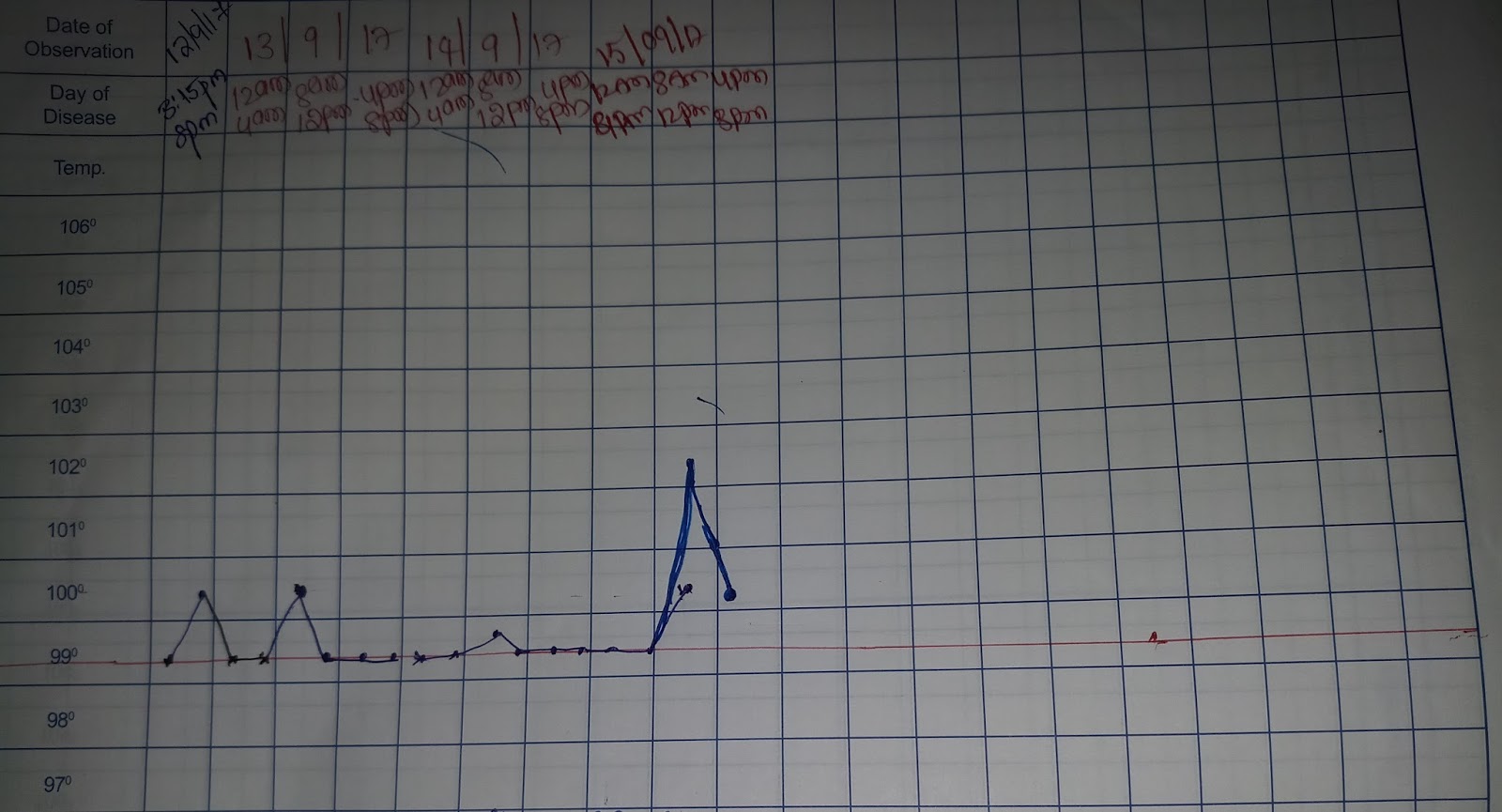
There were few spikes of fever, as shown below

Problem list and intervention:
- Child's spikes in fever are controlled by Tab.PARACETAMOL 500mg /QiD
- Tab. COTRIMOXAZOLE 80/400mg / BD is being given to tackle UTI
- Child complained of dry cough and cold. So, Syp.ASCORIL 2tsp/ TiD was given
- Child had one episode of vomiting and is complaining of nausea.
- Tab. ONDANSETRON 4mg/ BD is being given.
Currently, the fever spikes have reduced and recovery is expected soon.
Updates on any investigations and patient's outcome will be put up soon.
Above treatment was continued for two more days and the child recovered completely and was discharged.
Any suggestions or comments are highly appreciated. :)
Comments
Post a Comment